Not a trabecular shunt.
It does not depend on Schlemm's canal.
QMAX · Glaucoma
Equalizing pressure across the optic nerve head.
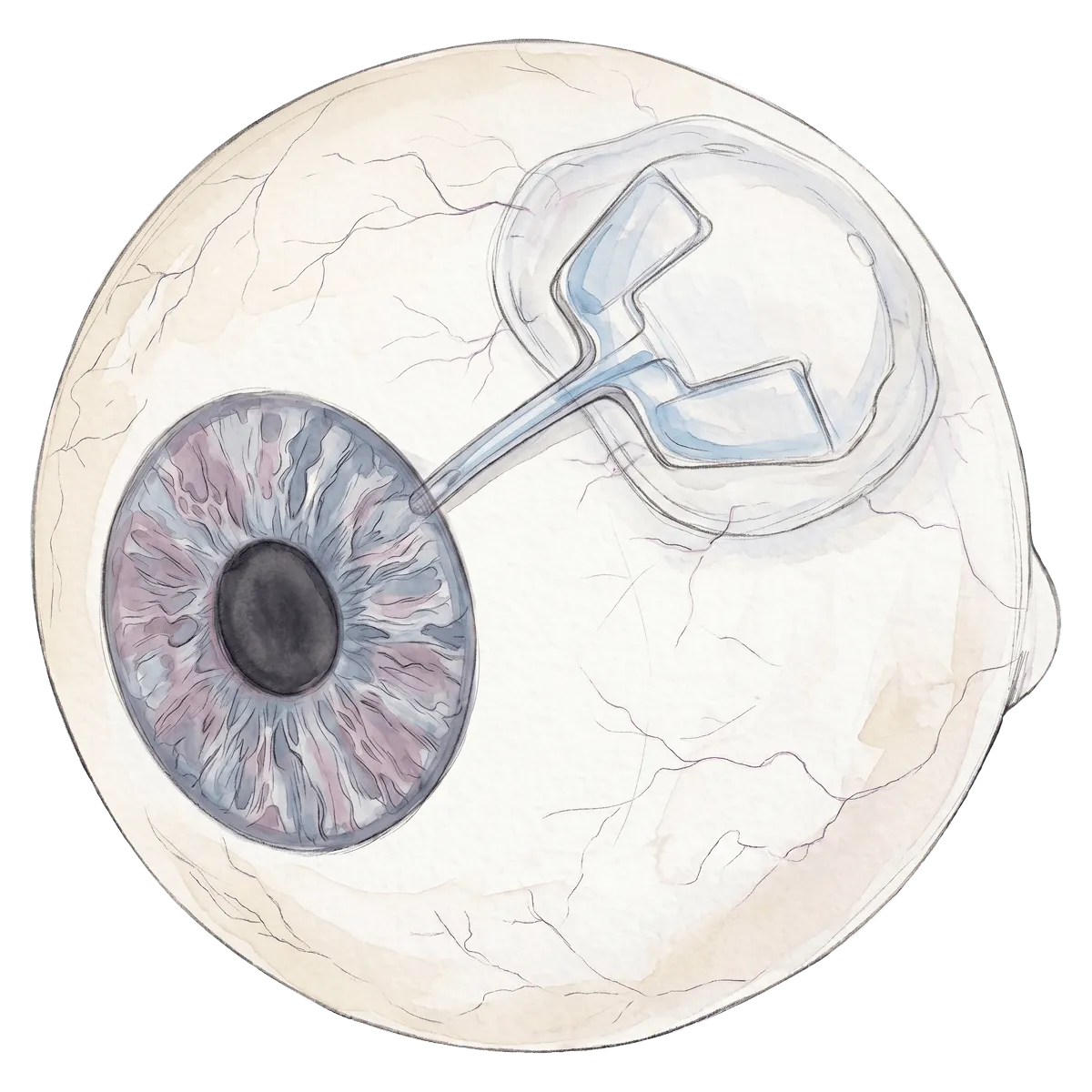
Glaucoma damages the optic nerve through a pressure gradient between the inside of the eye and the fluid around the nerve. QMAX is a first-in-class implant designed to neutralize that gradient.
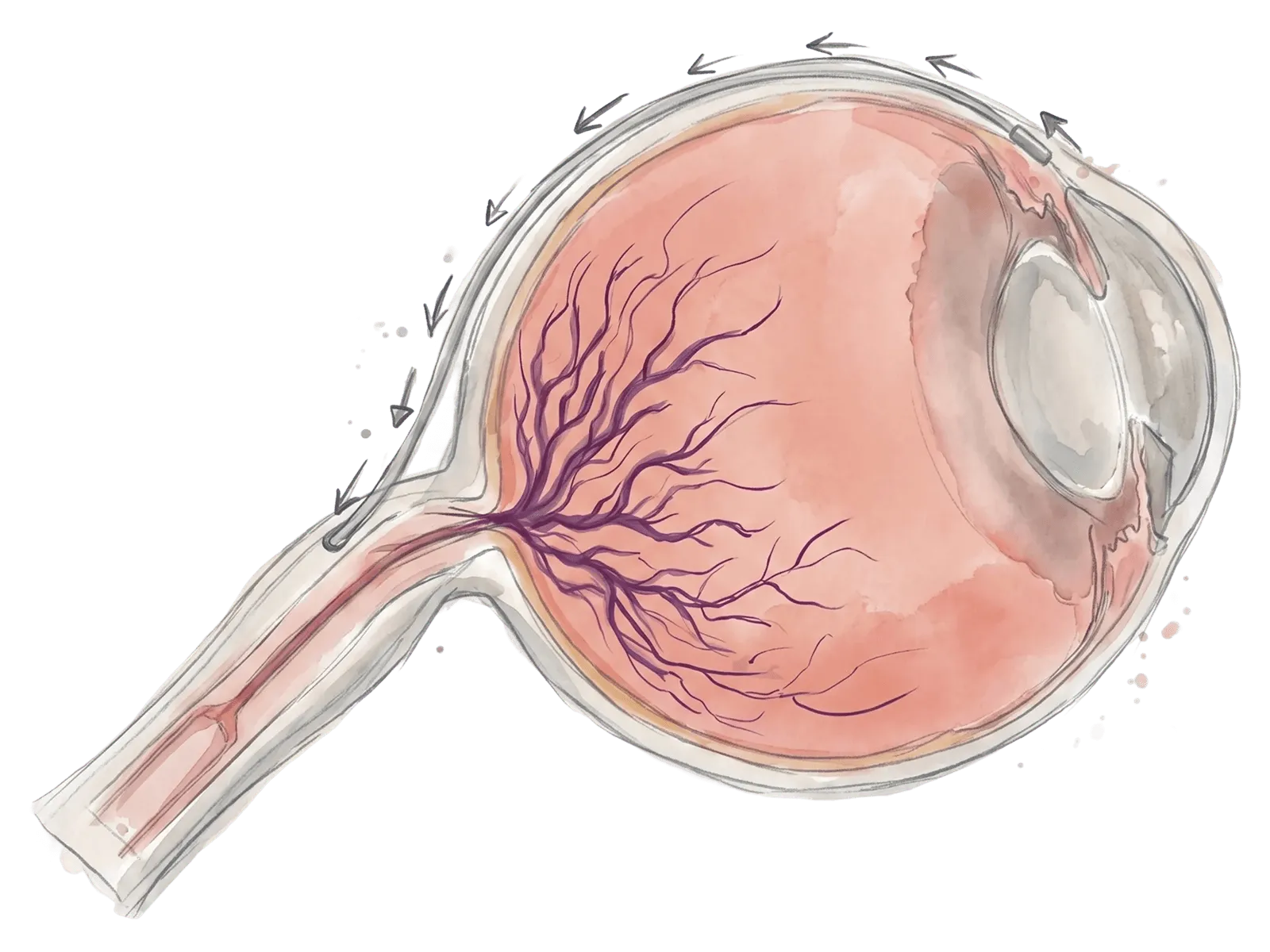
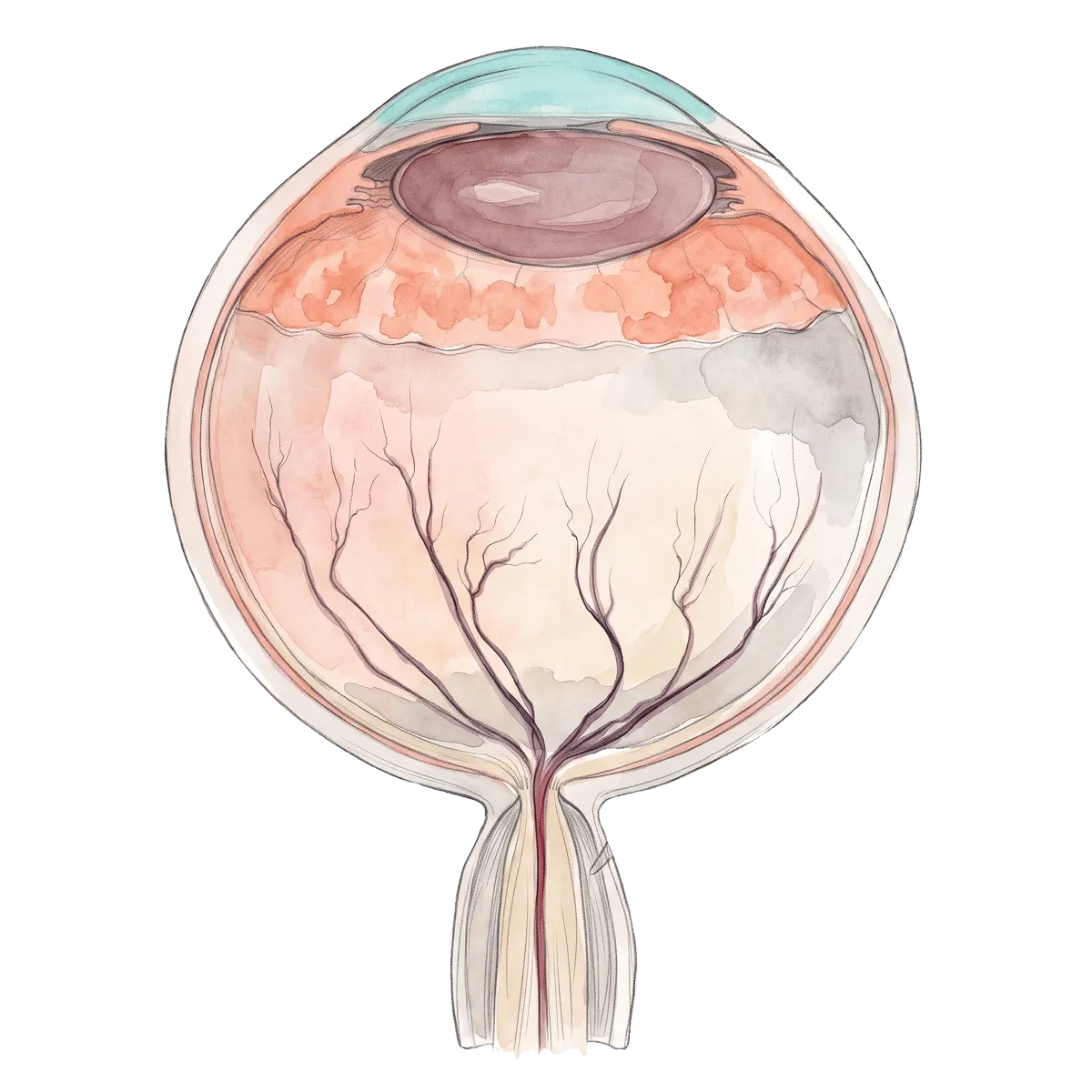
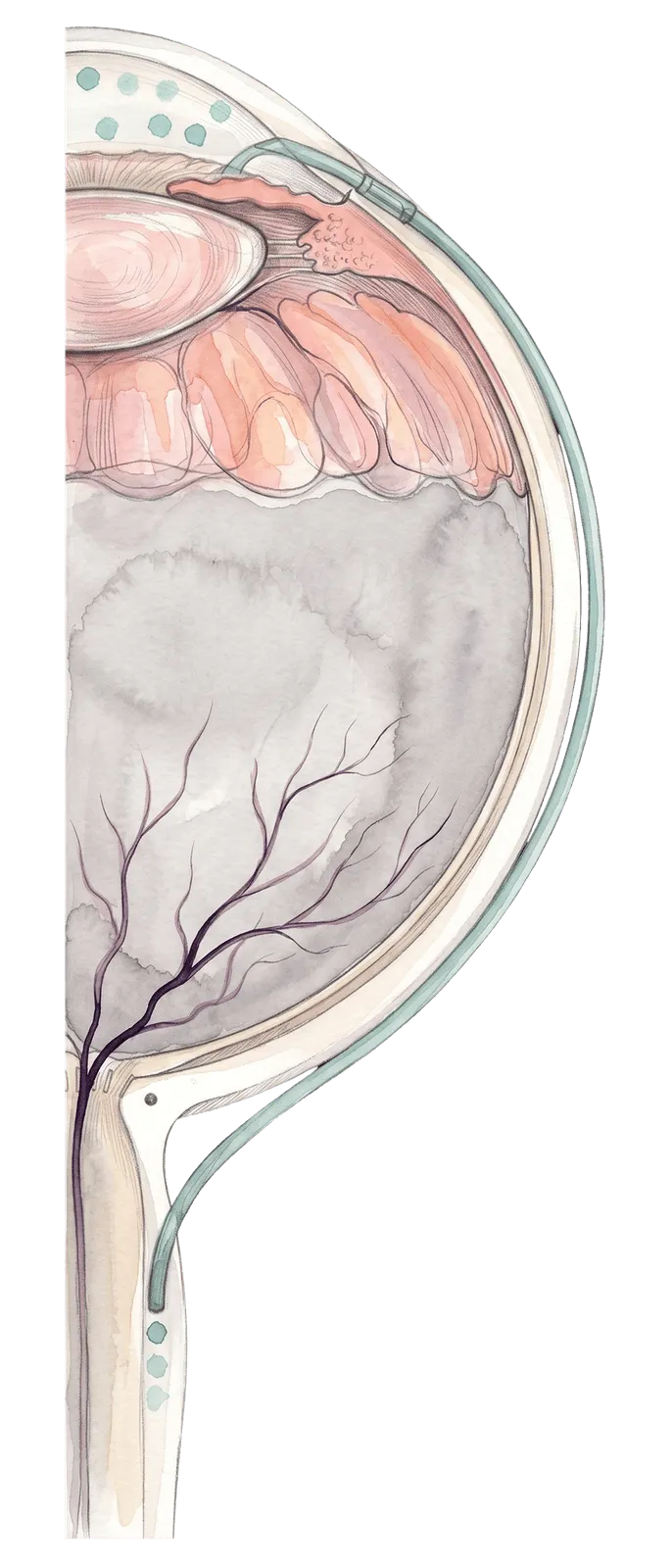
The optic nerve head sits at the lamina cribrosa, a thin sheet of nerve fibers under load from two sides: intraocular pressure (IOP) in front and the cerebrospinal fluid pressure in the space behind the nerve. What strains and damages the nerve is the difference between them, the translaminar pressure gradient. Lowering IOP alone narrows that gap from one side only. If the gradient remains, nerve fibers keep dying.
Connects the aqueous humor to the fluid space around the optic nerve
Equalizes pressure across the optic nerve head, not only inside the eye
Removes the gradient that strains and kills retinal ganglion cell axons
Operates without a filtering bleb and without anti-fibrotic agents
Targets both high-IOP and normal-tension glaucoma populations (investigator context; not labeling)
The result is a device that addresses what other surgeries leave on the table, including the patients whose vision keeps dropping at "normal" pressures.
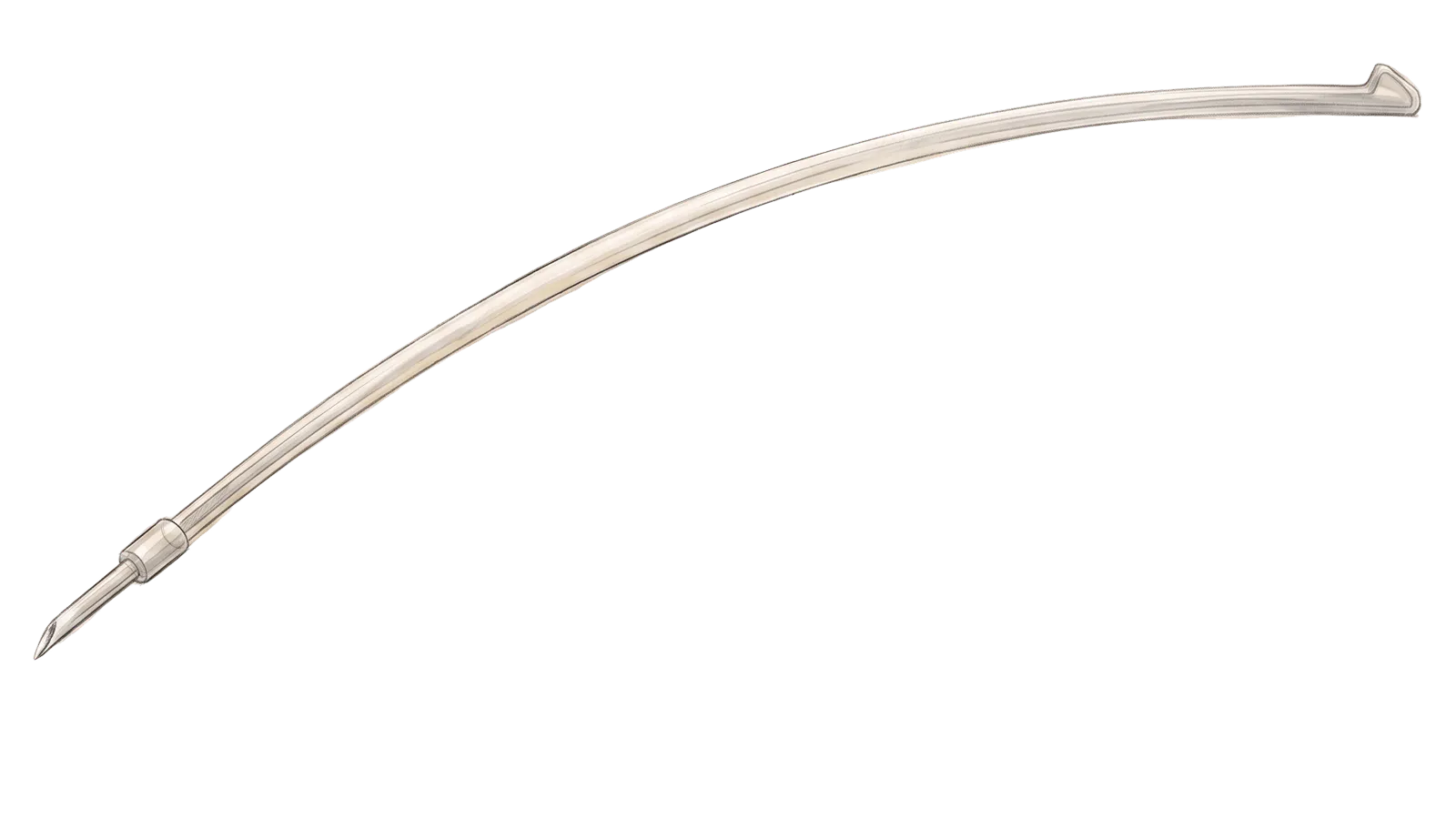
QMAX is delivered with QSCOPE, a single-use endoscopic system that gently tents the nerve sheath into a protected space and places the implant. It is designed as a simple, repeatable endoscopic procedure that integrates with existing cataract capital equipment, rather than a delicate open dissection.
Simple and repeatable
Endoscopic
High-turnover workflow compatible
Free of post-op bleb management
QMAX ships as a sterile, procedure-ready system: implant, delivery, and procedure pack designed for reproducibility and OR efficiency.
[alt pending: replace before launch] QMAX sterile packaging.
[alt pending: replace before launch] QMAX procedure pack contents overview.
QMAX is on a defined regulatory and clinical pathway toward US market access. The milestones below are forward-looking and subject to change; they are presented for investor and partner context, not as guarantees.
2026
FDA Breakthrough Device application (targeted)
2026
Gen 3 clinical study
2027
Endoscopic delivery feasibility study
2028
GLP preclinical · FDA IDE
2028–2030
Pivotal trial
2030
FDA approval (De Novo) (targeted)
John Berdahl, MDThe translaminar pressure gradient is the science glaucoma has been missing. QMAX is built directly on that foundation.
Richard Beckman, MDQMAX is transformational — a mechanism-led approach that addresses vision loss beyond IOP lowering alone.
Reay Brown, MDFrom a MIGS-era surgical perspective, QMAX is a credible next step for patients who still progress on conventional therapy.
10 global patent families covering the ONSAS mechanism, the device and delivery system, and the surgical method
First-in-human experience across three device generations, engineering out failure modes generation by generation
Clinical pathway routed through US sites